Pentoxifylline, the medicinal pillar of the PENTOCLO triad, has no longer been marketed in France for several months, but remains available abroad (Switzerland, Spain, England, USA, etc.).
The current alternatives would be: via ARSER, to make PENTOXIFYLLINE available to you (contact us) OR to offer a therapeutic alternative by substitution with a similar available drug.
To help patients who have undergone radiotherapy to minimize its after effects
Radiotherapy, After-effects, Means
What is radiotherapy?
Radiotherapy is a tool (local, such as surgery), essential to treat cancer. It is made with ionizing radiation and delivers an energy aimed at a specific tissue, in order to kill tumor cells.
Dr. Sylvie DELANIAN Oncologist Radiotherapist, St. Louis hospital:
Radiotherapy is a tool to treat cancer.
Unlike surgery, which uses a knife, the tool of radiation is energy that is introduced into a tissue and enables treatment; energy that is introduced; and as a result reduces an enemy, including cancer.
In cancer, radiotherapy is used for two things: it helps patients have less pain or less bleeding, this is called palliative radiotherapy; and radiotherapy, still the most “noble”, a curative radiation therapy that can cure 50% of cancers.
Without radiation therapy, there is no cure for cancer, obviously associated with surgery and/or chemotherapy. So, it’s an indispensable tool.
Download the transcript of the video (300KB)
What are the complications associated with radiotherapy?
Generally, patients are monitored regularly for five years. We are watching for a possible relapse of cancer or immediate complications from cancer treatments. Beyond that, patients are considered cured are rarely followed, yet they can still face more or less serious pathologies.
Dr. Sylvie DELANIAN Oncologist Radiotherapist, St. Louis hospital:
When we monitor the patients, generally five years, we’ll track down a possible recurrence or complication. Then the patients are free to leave, saying to themselves: we have taken back the daily routine of life; and it is then, that they are no longer assessed. And this is where a neuropathy of lower limbs will take five years to be diagnosed, heart disease or lung disease may never be diagnosed.
Dr. Pierre-François PRADAT Neurologist, La Pitié-Salpêtrière hospital:
The complications of radiotherapy teach us that these complications can occur years after the environmental aggression; so we understand the complexity of identifying the environmental factors in pathologies.
Dr. Sylvie DELANIAN Oncologist Radiotherapist, St. Louis hospital:
If there are patients that Americans call “long-term survivors” i.e. cured patients who live long, there can appear potential trouble in the area which received x-rays. For radiotherapy located exactly such as surgery, there may be consequences, positive or negative, but only in the area where we performed the radiation. As a result, there may be complications in connection with this treatment, not because someone was at fault or because of too much treatment but simply because all effective treatment can be sometimes dangerous.
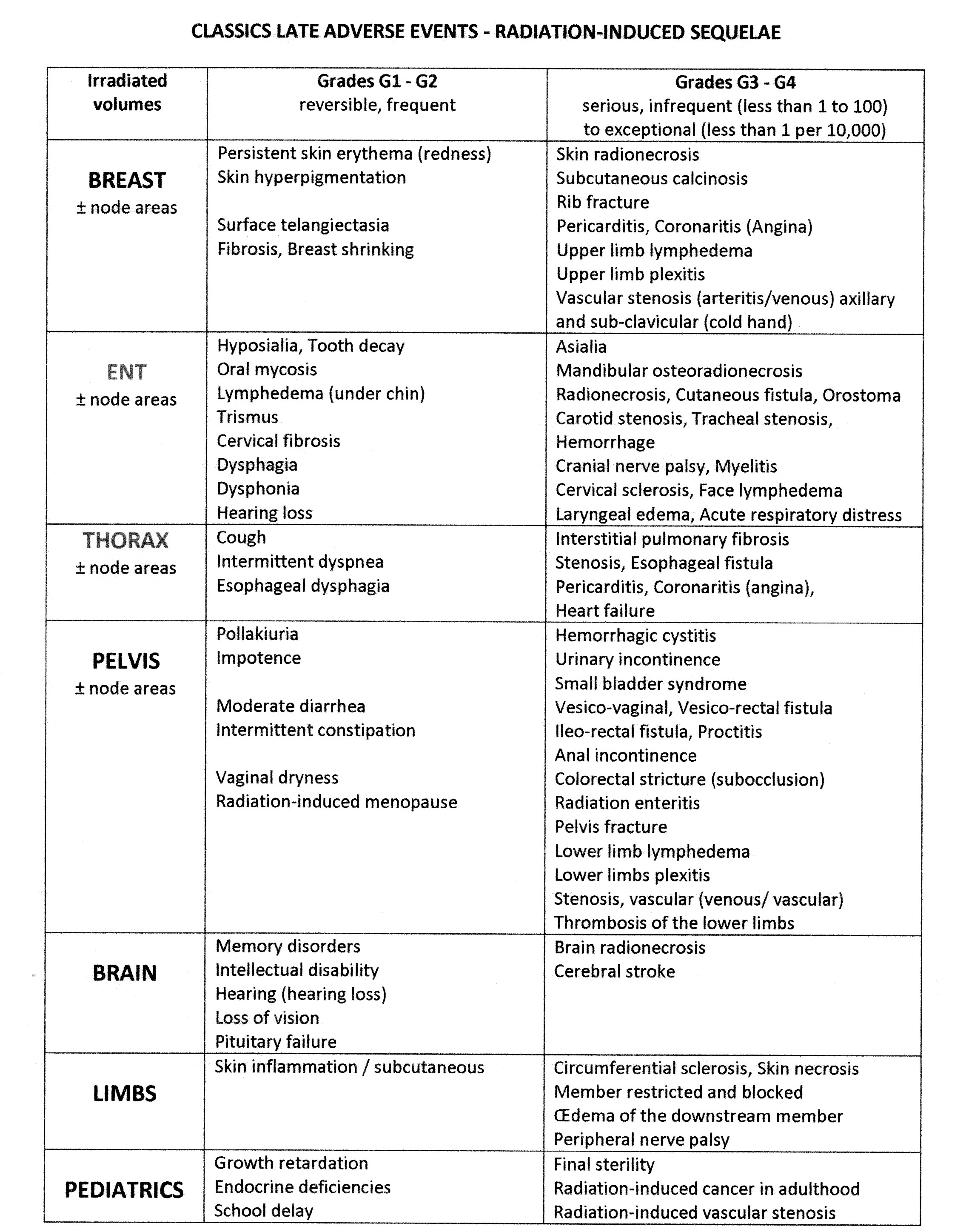
There are small after-effects, grade 1 or 2, extremely minor and fairly frequent. Take the example of breast cancer. A breast a little more pigmented which will be retracted, which is not annoying for life and which will simply leave a scar. However, serious complications I was telling you about earlier, that may occur and which are called sequels, can exist, but from a few months to a few years later, even 5 years, 10 years, 15 years, 30 years after radiation therapy. For irradiation concerning the internal mammary chain, there were, for example, cardiac complications that have been observed in recent years, or for a radiation to the Axilla and sub-clavicular, radio-induced plexopathies. It is exceptional, but it exists. Other complications can be observed, minor or major, in other organs. For example, pelvic irradiation for cancer of the rectum, prostate or the collar, a frequent event is the presence of digestive disorders. Minor, a seat or two a day a little more liquid, major, this may be an occlusion. Therefore, any minor or major event can exist. Major events are very rare but when they do occur are interesting and have nothing to do with an accident.
Dr. Pierre-François PRADAT Neurologist, La Pitié-Salpêtrière hospital:
The nervous system is very sensitive to radiotherapy. I would say, it is not so much the nerve cells that are themselves sensitive, it is rather the cells that surround them. We know that for the neurons to work, they need to be vascularized to receive oxygen. They need to protect themselves against infections, so there are special cells for it. And then there are support cells. The nervous system works in a network, so it needs an environment that allows it to maintain the architecture of this network. What happens after radiation therapy, is that this environment of neurons will be disorganized. Then we have, including a decrease in vascularity, neurons no longer having enough oxygen to operate. And all around this neuron will form what is called fibrosis. Fibrosis is like a scar, which will compress the neurons and that will prevent them from being able to push back, because these neurons have an intrinsic ability to reissue extensions, somewhat like the branches of trees they would cut, and well, this fibrosis will create a physical barrier that prevents regrowth of axons. I would say that these are the main effects of radiotherapy, although we still need to do a lot of basic research to understand all the mechanisms.
Download the transcript of the video (306KB)
Are these effects irreversible?
A dogma is widespread among doctors, in the light of previously taught knowledge, according to which (especially neurological) radiation-related injuries are irreversible. This dogma is false since there have appeared, since more than 10 years ago, new treatments that enable to reduce the consequences.
Dr. Sylvie DELANIAN Oncologist Radiotherapist, St. Louis hospital:
So far, it was considered that the sequel of radiotherapy was a scar, as in surgery, and that any scar was, by definition, irreversible. And here, let me make a personal digression, but I gave myself as objective, twenty years ago, to transform the word ‘irreversible’ to ‘reversible’ or at least to try.
This is the reason why I joined researchers at the Atomic Energy Commission to understand the mechanisms – it’s called the pathophysiology – and sought to dismantle the mechanisms in the form of several steps, like stair steps, saying and if we move to such place it can become… and there was a result. Of course, we did not convert with a magic wand, but we can get 50, 80, 90% of correct answers, i.e. people who will be transformed in their lives with a reduction in the aftermath. I think of necrosis in the mouth after ORL cancer. Properly treat this necrosis which disappears in 3 to 6 months instead of staying forever, it is interesting. And there are other examples. There are treatments that have been proven recently. I have the pleasure of leading the unit that I’ve developed at the Saint-Louis hospital and there are others which are in progress and there are very few centers who are interested, but there are some, which would require perhaps some assistance, infrastructure and personnel to go faster.
Dr. Pierre-François PRADAT Neurologist, La Pitié-Salpêtrière hospital:
We know that dogma spread, even among doctors, this dogma “nerve damage following radiotherapy are irreversible, this dogma is wrong. We have known for long that the neurons, particularly in the nervous system peripheral in the central nervous system is complicated, but neurons have an intrinsic ability to regenerate. In practice, in fact, we’re working very transverse from experimentation to therapeutic or diagnostic applications in humans. I can quote a number of works. One of the challenges is to detect early complications of radiotherapy. And so far, this isn’t the case. In fact, the diagnosis is often late, and unfortunately, patients follow a long medical journey with multiple consultations until “complication of radiation therapy” is finally diagnosed. And it’s a real loss of opportunity for patients, as now, we are moving toward treatments that are protective treatments that are more likely to work and that the disease will be taken early.
Download the transcript of the video (303KB)
Classics late adverse events – Radiation-induced sequelae
France has abilities, researchers – including young researchers – but unfortunately, she has no budgets. In addition, this issue is still considered to be a “customer service” not noble enough.
Dr. Sylvie DELANIAN Oncologist Radiotherapist, St. Louis hospital:
All these works are ongoing because they are supported by the goodwill of individuals who met and decided to address a problem to try to limit the suffering of patients. Compassion, it’s our job, but… to go beyond.
Dr. Pierre-François PRADAT Neurologist, La Pitié-Salpêtrière hospital:
We have the ability, we have researchers, we meet young researchers who would like to work on this area permanently, unfortunately there are no budgets. It’s sad, but they will work in other laboratories on subjects that are more fashionable, for which it is easier to find research grants.
Dr. Sylvie DELANIAN Oncologist Radiotherapist, St. Louis hospital:
You have to have a few more working with means.
Dr. Pierre-François PRADAT Neurologist, La Pitié-Salpêtrière hospital:
And then in our areas that are neurological diseases, there is the issue of disability. And patients who have difficulties, on the day for things that seem the simplest of everyday life. So it is a duty to help them, and I would say that it is a duty to help them regardless of their geographical origin and regardless of their social status so that they can all benefit from aid schemes, which incidentally, sometimes exist but which are not well known and for which networks are insufficiently developed.
Download the transcript of the video (302KB)
Nous utilisons des cookies pour vous garantir la meilleure expérience sur notre site notamment au niveau de la sécurité. Ils ne sont pas utilisés à des fins commerciales. Si vous continuez à utiliser notre site, nous considérerons que vous acceptez l'utilisation des cookies. S'ils ne sont pas activés sur votre navigateur, vous pourriez ne pas avoir accès à certaines fonctionnalités (l'annuaire par exemple). Vous trouverez sur ce lien la méthode pour les activer pour notre site. Merci de votre compréhension.Ok
{kind=link}